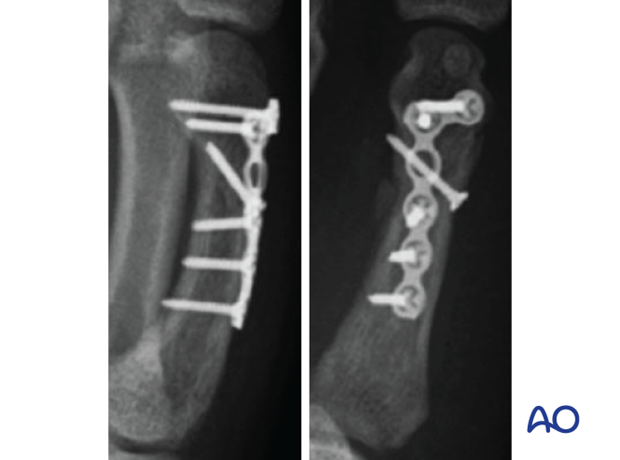
Lag-screw fixation with a neutralization plate
1. General considerations
Principles
In short oblique fractures, only one lag screw can be inserted. This is insufficient to produce enough stability, and the lag screw must be protected by a plate. A neutralization plate may also be indicated if screw fixation alone is not providing sufficient stability, eg, in poor quality bone.
As the screw should be inserted perpendicularly to the fracture plane, in most cases, it has to be inserted independently of the plate.

Plate selection
Select a plate (1.5–2.0 mm) according to the size of the bone, fracture geometry, and surgeon’s preference.
The plate length should allow for at least two screws in each main fragment.
The plate is available as a conventional compression plate or with variable-angle (VA) locking-head screws.

AO teaching video
Metacarpal III–Short oblique fracture–Fixation with a 2.0 mm lag screw and 2.0 mm Variable Angle Adaption plate
2. Patient preparation
Place the patient supine with the arm on a radiolucent hand table.

3. Approaches
For this procedure, the following approaches may be used:
In the 2nd metacarpal, a radial approach may be used. In the 5th metacarpal, an ulnar approach may be used.
4. Reduction
Indirect reduction by traction
Reduce the fracture with longitudinal traction on the finger and pressure from a periosteal elevator or a dental pick.

Direct reduction
Secure the reduction with pointed reduction forceps and confirm reduction with an image intensifier. Ensure the reduction forceps do not conflict with the planned screw position.
It is essential to confirm that the apex of each fracture fragment has been properly reduced.

Alternatively, special reduction forceps designed for percutaneous fixation may be used.

5. Checking alignment
Identifying malrotation
At this stage, it is advisable to check the alignment and rotational correction by moving the finger through a range of motion.
Rotational alignment can only be judged with flexed metacarpophalangeal (MCP) joints. The fingertips should all point to the scaphoid.
Malrotation may manifest by an overlap of the flexed finger over its neighbor. Subtle rotational malalignments can often be judged by a tilt of the leading edge of the fingernail when the fingers are viewed end-on.
If the patient is conscious and the regional anesthesia still allows active movement, the patient can be asked to extend and flex the finger.
Any malrotation is corrected by direct manipulation and later fixed. Flexing the MCP joints while preventing overlap of the fingers will reduce rotational displacement.

Using the tenodesis effect when under anesthesia
Under general anesthesia, the tenodesis effect is used, with the surgeon fully flexing the wrist to produce extension of the fingers and fully extending the wrist to cause flexion of the fingers.

Alternatively, the surgeon can exert pressure against the muscle bellies of the proximal forearm to cause passive flexion of the fingers.

6. Lag-screw fixation
Insertion of the lag screw
Insert the lag screw in the center of the fracture and perpendicular to the fracture plane. Carefully tighten the screw.
The fracture is now compressed. The reduction forceps may now be removed.
Confirm reduction and correct screw position with an image intensifier.

Screw size selection
The exact size of the diameter of the screws used will be determined by the fragment size and the fracture configuration.
The various gliding and thread hole drill sizes for different screws are illustrated here.

Screw length pitfalls
- Too short screws do not have enough threads to engage the far cortex properly. This problem increases when self-tapping screws are used due to the geometry of their tips.
- Too long screws endanger the soft tissues, especially tendons and neurovascular structures. With self-tapping screws, the sharp cutting flutes are especially dangerous, and great care has to be taken that the flutes do not protrude beyond the cortical surface.

Pitfall: screw too close to the fracture

Pitfall: beware of fissure lines

7. Plate fixation
Apply the neutralization plate dorsally.
Insert at least two screws proximally and distally to the fracture in neutral mode.
Cover the plate with periosteum to avoid adhesion between the tendon and the implant leading to limited finger movement.

8. Final assessment
Confirm correct rotational alignment by clinical examination.
Confirm anatomical reduction and correct placement of implants in AP, lateral, and oblique views.
9. Aftercare
Postoperative phases
The aftercare can be divided into four phases of healing:
- Inflammatory phase (week 1–3)
- Early repair phase (week 4–6)
- Late repair and early tissue remodeling phase (week 7–12)
- Remodeling and reintegration phase (week 13 onwards)
Full details on each phase can be found here.
Postoperative treatment
If there is swelling, the hand is supported with a dorsal splint for a week. This would allow for finger movement and help with pain and edema control. The arm should be actively elevated to help reduce the swelling.
The hand should be splinted in an intrinsic plus (Edinburgh) position:
- Neutral wrist position or up to 15° extension
- Metacarpophalangeal (MCP) joint in 90° flexion
- Proximal interphalangeal (PIP) joint in extension

The reason for splinting the MCP joint in flexion is to maintain its collateral ligament at maximal length, avoiding scar contraction.
PIP joint extension in this position also maintains the length of the volar plate.

After subsided swelling, protect the digit with buddy strapping to a neighboring finger to neutralize lateral forces on the finger.

Functional exercises
To prevent joint stiffness, the patient should be instructed to begin active motion (flexion and extension) immediately after surgery.

Follow-up
See the patient after 5 and 10 days of surgery.
Implant removal
The implants may need to be removed in cases of soft-tissue irritation.
In case of joint stiffness or tendon adhesion restricting finger movement, arthrolysis or tenolysis may become necessary. In these circumstances, the implants can be removed at the same time.











