Dorsoulnar approach to the 5th metacarpal
1. Indication
This approach is indicated for extraarticular fractures of the 5th metacarpal, especially for extraarticular neck fractures.
It avoids conflict with the extensor mechanism of the metacarpophalangeal (MCP) joint.
2. Surgical anatomy
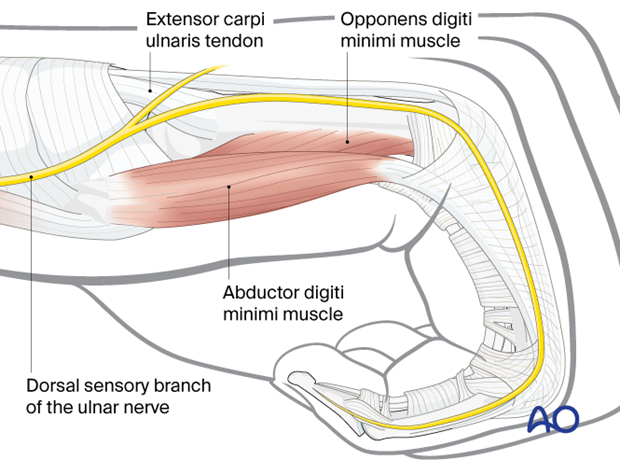
The insertion of the extensor carpi ulnaris tendon is onto the ulnar base of the 5th metacarpal.
The dorsal sensory branch of the ulnar nerve crosses over the base of the 5th metacarpal.
3. Skin incision
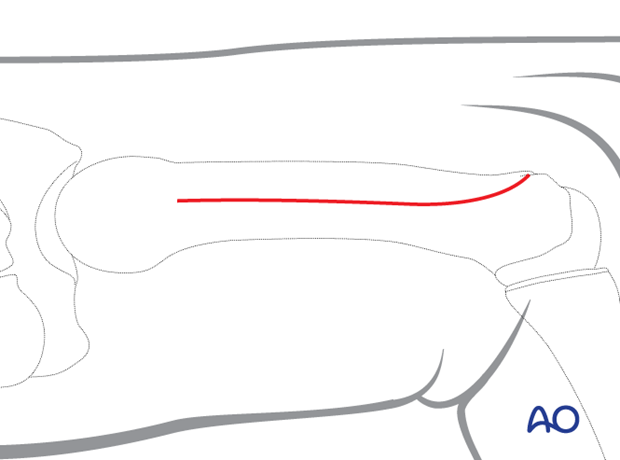
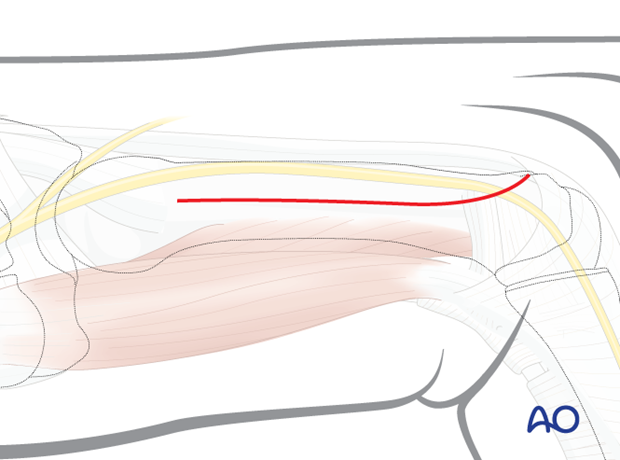
Start the incision distal to the metacarpal base, lateral in line with the diaphysis.
Continue the incision with a slight dorsal curve as far as the metacarpal head. This will avoid damage to the ulnar collateral ligament and the sagittal band of the extensor mechanism.
4. Exposure of the diaphysis
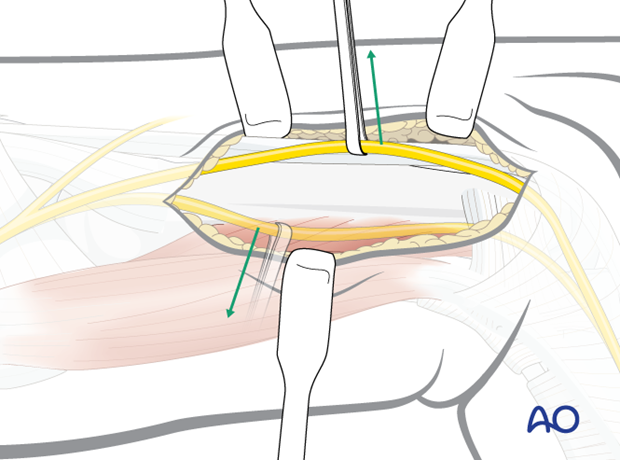
Be aware of the dorsal sensory branch of the ulnar nerve in the subcutaneous tissue. Mobilize the nerve so it can be moved dorsally and/or palmarly to gain access for plate and screw insertion.
Expose the diaphysis down to the bone.
5. Wound closure
Cover the implant with the periosteum as far as possible; this helps minimize contact between the extensor tendons and the implant.
If an intertendinous connection has been cut, it should be repaired.












