Plating
1. General considerations
Introduction
Articular fractures, simple or comminuted, of the 2nd and 5th metacarpal base may be fixed with a T- or Y-plate.
The articular fragments are reduced and fixed using the transverse part of the plate. In the second step, the extraarticular fracture component is reduced and fixed.
Noncomminuted fracture components, eg, between the articular fragments or between the articular block and the diaphysis, may be fixed with compression.
If the articular fragment cannot be reduced or are too small to be fitted with a plate, conversion to arthrodiastasis should be considered.

Plate selection
Select a plate according to the size of the bone, fracture geometry, and surgeon’s preference. A T-shaped plate may be used. Other shapes may also be applied.
A plate with variable-angle (VA) locking-head screws has the advantage to allow insertion of two or three screws in variable angles into the articular block. The rounded plate edges avoid soft-tissue irritation and adhesion.
The plate needs to be contoured to fit the anatomy of the end segment.

Associated dislocation of the 4th metacarpal
Fractures of the 5th metacarpal base may be associated with a carpometacarpal (CMC) joint dislocation of the 4th ray. In that case, the 4th metacarpal is reduced first and usually stabilized with K-wire transfixation.
Occasionally, there is a subluxation of the 3rd metacarpal or even the 2nd metacarpal, and any combination of additional fractures can be seen.
Once the dislocation of any other CMC joint has been stabilized, fixation of the fracture may proceed.

2. Approaches
For this procedure, the following approaches may be used:

3. Reduction and fixation of the articular block in a simple T- and Y-shaped fracture
If the fracture line allows, eg, in a T- or Y-shaped fracture with the articular fracture line running from palmar to dorsal, a lag screw may be inserted to stabilize the articular fracture. This converts a three-part fracture to a two-part fracture.
Make sure the screw track is not interfering with later plate application.

4. Reduction of a comminuted fracture
Restoration of length
Apply axial traction on the finger, either manually or with a finger trap.

A small external fixator can be used, with K-wires inserted into the hamate and the distal metacarpal, preliminarily to align the ray and allow anatomical reduction of the joint surface.
The external fixator can be removed after finalizing plate application.

As an alternative to external fixation, a temporary K-wire may be inserted through the shaft and into the adjacent noncompromised metacarpal to maintain length and alignment. This K-wire can be removed after finalizing plate application.
Accompanying hamate fracture
If there is a shearing fracture of the hamate, reduce this fragment first and fix it with a lag screw.

Reduction of fragments
A capsulotomy is needed to check the reduction of the articular fragments if the joint capsule is not already ruptured.
Use a dental pick, periosteal elevator, or small K-wires to reduce the fragments. Insert small K-wires for preliminary fixation of these articular fragments. Occasionally, these K-wires are inserted percutaneously. Make sure not to injure the dorsal sensory branch of the ulnar nerve.
Check reduction with an image intensifier.
If the hamate is uninjured, its articular surface can be used as a template for restoring the articular surface of the metacarpal base.

Buttressing small fragments
Additionally, a periarticular K-wire may be used to reposition and support impacted articular fragments.
The end of the K-wire may protrude through the skin, which facilitates removal after consolidation of the fracture.

Bone graft
If conventional condylar plates are used, cancellous autograft, or very occasionally bone substitutes (eg, hydroxyapatite, tricalcium phosphate), will be necessary to support the articular fragments and fill the impaction void. Bone graft will enhance the healing process.

5. Checking alignment
Identifying malrotation
At this stage, it is advisable to check the alignment and rotational correction by moving the finger through a range of motion.
Rotational alignment can only be judged with flexed metacarpophalangeal (MCP) joints. The fingertips should all point to the scaphoid.
Malrotation may manifest by an overlap of the flexed finger over its neighbor. Subtle rotational malalignments can often be judged by a tilt of the leading edge of the fingernail when the fingers are viewed end-on.
If the patient is conscious and the regional anesthesia still allows active movement, the patient can be asked to extend and flex the finger.
Any malrotation is corrected by direct manipulation and later fixed. Flexing the MCP joints while preventing overlap of the fingers will reduce rotational displacement.

Using the tenodesis effect when under anesthesia
Under general anesthesia, the tenodesis effect is used, with the surgeon fully flexing the wrist to produce extension of the fingers and fully extending the wrist to cause flexion of the fingers.

Alternatively, the surgeon can exert pressure against the muscle bellies of the proximal forearm to cause passive flexion of the fingers.

6. Plate preparation
Plate trimming
Adapt the plate length to the length of the metacarpal. Avoid sharp edges, which may be injurious to the tendons. There should be at least 3 plate holes distal to the fracture available for fixation in the diaphysis. At least two screws need to be inserted into the diaphysis.

Contouring
Contour the plate exactly to fit the surface of the metacarpal, including any necessary twisting.

7. Bridge plating
Plate positioning
Place the plate exactly so that the articular fragments can be fixed using screws through the proximal plate holes. Often, it is not possible to insert a screw into each fragment. Small fragments should be supported by adjacent large fragments or bone graft.
Be careful to ensure that the screws do not perforate the joint surface.
Keep the plate in place with the atraumatic forceps.

Begin fixation with the most critical articular fragment.
Drill carefully not to displace the fragments and penetrate the articular surface.
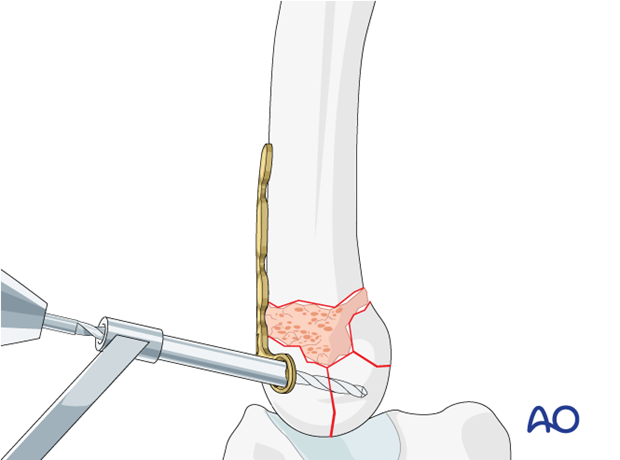
Insert the first screw.
Confirm the reduction and correct screw position using image intensification.

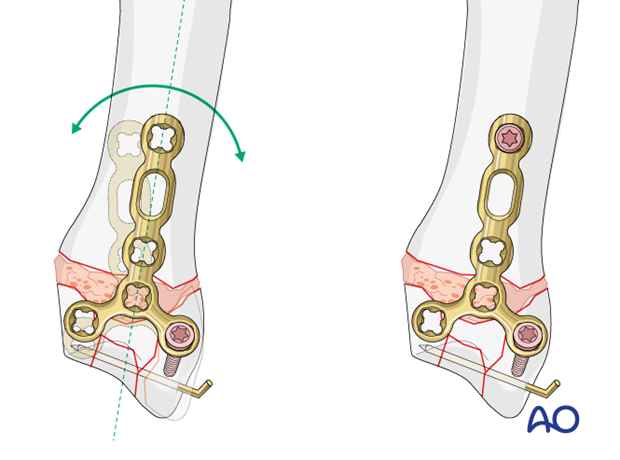
Align the plate along the shaft and bring the bone out to length.
Insert the VA locking head screws into the diaphyseal part of the plate without compression.
Check rotational alignment clinically and with an image intensifier.
Insert the second VA locking screw in the other end of the T-shape.
Extrinsic compression
If the articular fracture allows, apply extrinsic compression.
Compress the fracture with reduction forceps. Position one tip of the forceps on the plate with the first screw to avoid damage of the bone cortex.
Insert the second VA locking screw to hold the compression.

Sagittal articular fracture of the 5th metacarpal base
It is helpful to apply the T-plate ulnarly to allow for extrinsic compression with reduction forceps of a sagittal articular fracture and hold the compression with the proximal VA locking-head screws.

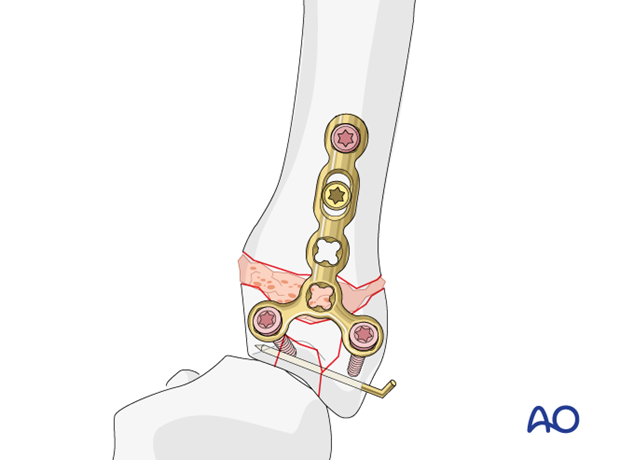
Insertion of further diaphyseal screws
Insert the second and, if possible, a third screw into the diaphyseal fragment and tighten them.
When the fixation is completed, remove the external fixator and K-wires, other than those needed to buttress small articular fragments.
Cover the plate with periosteum to avoid adhesion between the tendon and the implant leading to limited finger movement.
Fixation of further fragments
If additional large metaphyseal fragments need fixation, insert screws through the plate, or insert an independent lag screw.
If needed, use additional bone graft to fill any defect.

8. Compression plating of a simple metadiaphyseal fracture
Insert the first cortical screw in the oblong hole in compression mode to compress the extraarticular fracture component.
Check again rotational alignment clinically and with an image intensifier.
Insert a second screw into the diaphyseal segment to finalize the fixation.

9. Final assessment
Confirm correct rotational alignment by clinical examination.
Image intensification may be used to confirm anatomical reduction and correct placement of implants in two views.












