Approach to the anteromedial tibial surface
1. Introduction
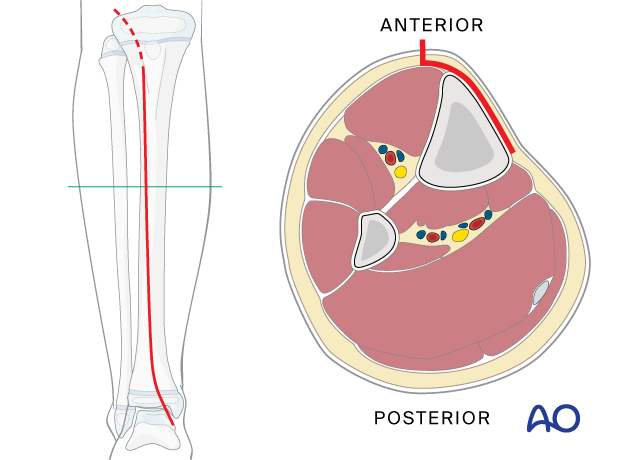
The anteromedial approach to the tibial shaft is performed through an incision placed just lateral to the anterior tibial crest.
It is most commonly used for fractures of the distal third of the tibial shaft. However, it can be used to expose the entire anteromedial surface.
It is also useful for debridement and irrigation of open fractures when an incision on the subcutaneous surface should be avoided.
The advantages of this approach are:
- It removes no muscle from the fracture fragments.
- The relatively simple shape of this surface facilitates plate contouring.
This approach should not be used when there is substantial contusion of the medial skin.
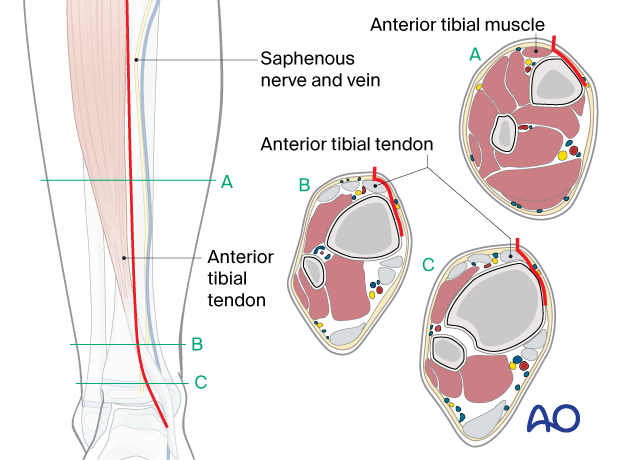
2. Anatomy
The triangular shape of the tibia
The lateral and posterior surfaces of the tibia are covered by muscle. The anteromedial surface has only a thin layer of subcutaneous tissue and skin. This surface provides less blood supply to the underlying bone.
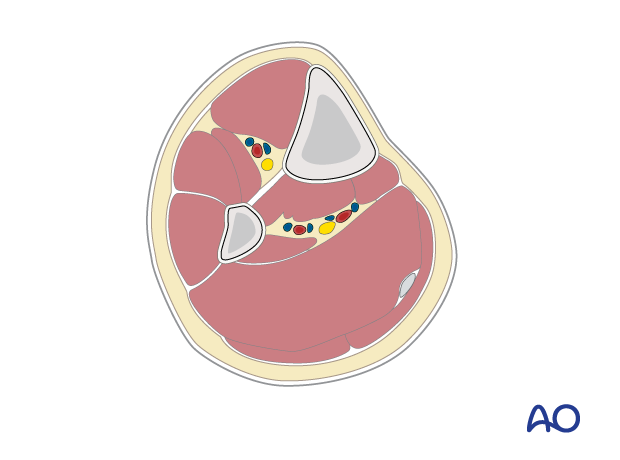
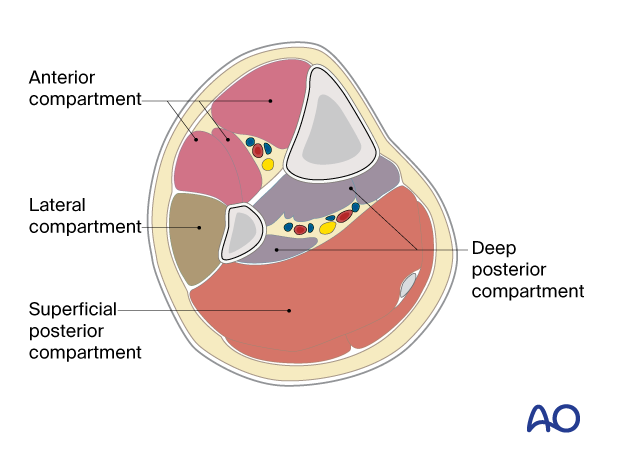
Compartments
The lower leg has four compartments.
The anterior compartment contains:
- Tibialis anterior
- Extensor hallucis longus
- Extensor digitorum longus
- Anterior tibial artery
- Deep peroneal nerve
The lateral compartment contains:
- Peroneus longus
- Peroneus brevis
- Superficial peroneal nerve
The deep posterior compartment contains:
- Tibialis posterior
- Flexor hallucis longus
- Flexor digitorum longus
- Peroneal artery
- Posterior tibial artery
- Tibial nerve
The superficial posterior compartment contains:
- Gastrocnemius
- Soleus
- Sural nerve
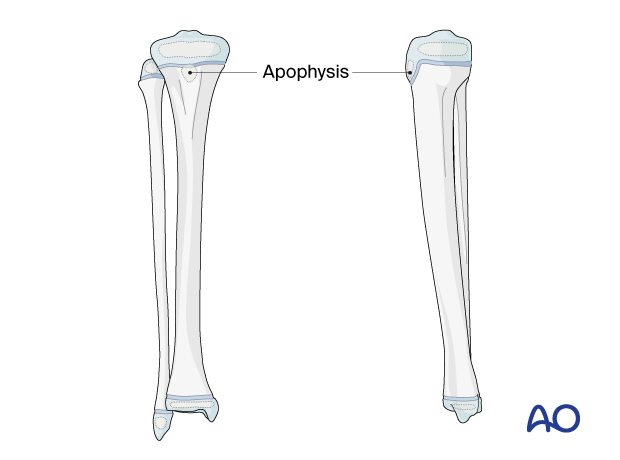
Proximal and distal tibial physes
The physis at each end of the tibia must be protected during surgical approaches and implant application.
The proximal tibial physis extends anteriorly and distally as an apophysis, which forms the tibial tuberosity.
This may be damaged as a consequence of injury and surgery, leading to tibial deformity.
3. Skin incision
Identify the level of the physis with image intensification and mark this on the skin before making an incision.
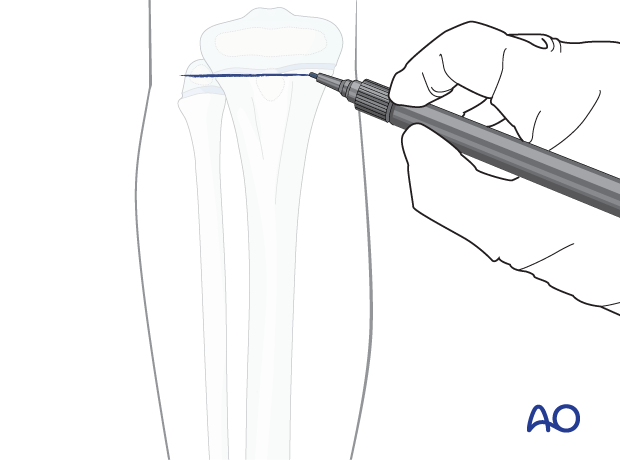
Approach the anteromedial surface through a longitudinal incision, 1–2 cm lateral to the tibial crest. Continue the incision distally along the medial edge of the tibialis anterior with a gentle curve toward the medial malleolus.
The deep dissection should remain superficial to the fascial layer of the anterior compartment.
Periosteal stripping or compression should be avoided whenever possible.
The length of the incision depends on the planned plate length.
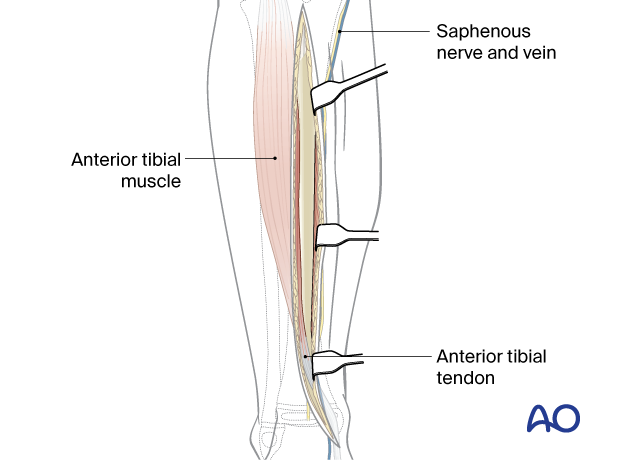
Take care not to injure the saphenous vein and nerve, which are at risk at the distal extent of the approach.
Perforation of the anterior tibial tendon sheath should be avoided, as this can cause adhesions.
4. Dissection
Mobilize full-thickness skin and subcutaneous tissue flaps in a medial direction to directly expose the anteromedial aspect of the tibia.
Leave the periosteum intact if possible.
It may be necessary to reflect periosteum from the fracture edges to achieve a direct anatomical reduction, but this should be done cautiously.
Make sure not to damage the perichondral ring at either physis.
5. Wound closure
The skin and subcutaneous tissues are closed according to surgeon preference.
The fascia should be left open to minimize the risk of compartment syndrome.











