Plate fixation
1. Preliminary remarks
Fractures of the proximal 5th metatarsal (Jones and Jones variants) can be treated with plates.
Plate selection is based upon the size of the proximal segment.
A straight locking or nonlocking plate may be used for larger extraarticular fragments.

Anatomical considerations
Proper alignment of the metatarsal heads is a critical goal in restoring the forefoot mechanics.
A normal curved “cascade” (Lelièvre’s parabola) appearance, which is symmetric with the other foot, is mandatory on the AP view. See illustration. This symmetry ensures that the normal length of the metatarsal is restored.
It is also critical to restore the metatarsals in their axial or horizontal plane so that all the metatarsal heads are on the same level in the axial view.
Any malalignment, particularly flexion, will recreate focally high pressure during the stance phase and toe-off, resulting in pain and subsequent callus formation.
The sesamoids, rather than the first metatarsal head, bear weight in the first row. Therefore, one must look at the sesamoid level in establishing the alignment in the axial or horizontal plane of the first metatarsal.

Timing of surgery
The timing of surgery is influenced by the soft tissue injury and the patient's physiologic status.

2. Patient preparation
This procedure is typically performed with the patient placed supine with the knee flexed at 90°.

3. Approach
Most of these fractures can be fixed with percutaneous screw fixation.
The fracture can be accessed through a lateral approach to the fifth metatarsal when an open procedure is needed.

4. Reduction and preliminary fixation
Expose the fracture with minimal soft-tissue dissection off the bone.
Clean out any avascular tissue to allow reduction.
Reduce the fracture with the help of a reduction forceps and provisionally fix it with one or two 1.6 mm K-wires or reduction clamps.
Anticipate the plate position when placing the K-wires to avoid interference.

5. Fixation with straight plate
Insert two or three screws through the 2.0 plate into the proximal fragment.

Use a small clamp to stabilize the fracture.
Attach a small bone hook in the distal hole of the plate and apply distal traction to the plate creating compression at the fracture site.
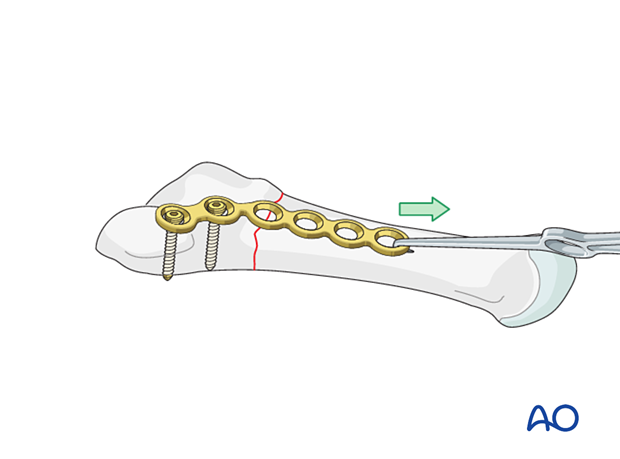
Insert two or three bicortical screws through the plate into the distal fragment.
6. Aftercare
An appropriate well-padded dressing should be applied to protect the surgical incision. Compression will help control swelling.
If present, the skin-pin interface should be similarly well-padded but with dressings that can be readily removed to inspect for pin site infection.
Immediate postoperative treatment is rest, ice, and elevation.
The patient should restrict weight-bearing for six weeks until signs of radiographic healing are present. After this, patients can be weight-bearing as tolerated.
Patients must exercise their ankle and subtalar joints out of the orthosis to prevent stiffness (eg, by stretching their Achilles).
X-ray the metatarsals at six weeks to confirm satisfactory union and remove K-wires if present. Once the fracture is united, the orthosis may be gradually discontinued.
A gastrocnemius release may need to be performed in cases with postoperative gastrocnemius contracture. This occurs more typically in the mid- and hindfoot.
If the gastrocnemius muscle has been released, a splint or cam walker can be used to protect the surgical site.











